Delivering intake and assessment
Initial Assessment and Referral - Decision Support Tool
Medicare Mental Health provides navigation to local services and supports that best suit a consumer, based on their presenting treatment needs and recovery goals.
The best way to explore their presenting needs/risks and preferences, is through the completion of the Initial Assessment and Referral Decision Support Tool (IAR-DST).
When not to undertake an IAR-DST
Most calls to Medicare Mental Health will require an IAR-DST to be undertaken.
The following are examples of when it may not be necessary to utilise the IAR-DST.
- The caller is seeking information or resources only.
- The caller seeking information about relevant or local services only.
- An initial assessment has already been undertaken (e.g. by a referrer) and the level of care required has been identified. In this instance, referrer, consumer, carer, family member, or friend may simply require support identifying an appropriate local service (navigational supports only).
- The consumer does not give consent for an IAR assessment.
- The consumer is identified as requiring immediate referral to specialist, acute or emergency services (the IAR-DST can also guide this decision).
Accessing the IAR-DST form
To access the IAR-DST you must create a Contact and convert to a Client record. At the bottom of the Client screen, click on the "Data for Intake" button.

Referral Origin
When an IAR-DST call has been directly set up by a third-party referrer (such as a General Practitioner (GP) or support worker), or the IAR-DST is taken from a parent of an underage child, Guardian or Power of Attorney, that third party involvement should be listed on the webform as the referrer. The referrers details need to be recorded on the webform or the referral will not progress to the next stage. If details are unknown, write ‘unknown’.
The fields in the ‘Referrer section’ are mandatory:
- Referrer profession
- Referrer first name
- Referrer last name
- Referrer organisation
Upload a document
For guidance on uploading files/documents, see the Additional documentation section.
Referral criteria to Levels of care
Sitting behind the assessment domains is an algorithm that leads to a recommended level of care.
As the domains are interactive (in that each of the assessment factors can interact with judgements on other domains) there is considerable complexity in the possible combinations. The suggested referral criteria aim to simplify the approach by focusing only on the main patterns of presenting problems likely to be found in primary mental health care. It is important to emphasise that the proposed referral criteria are offered only to guide judgements about the likely best treatment option.
Each presenting individual will have unique requirements that must always take precedence in decision making.
The option to ‘override’ the DST level of care has been built into the webform. A decision to override the DST can be based on clinical judgement, and consumer choice.
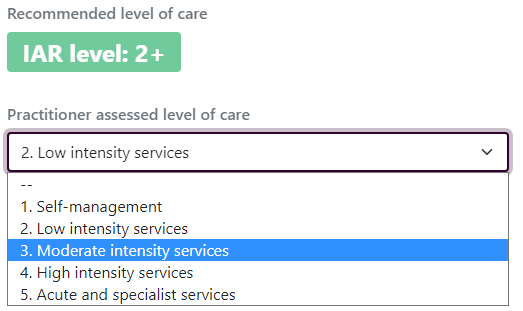
IAR-DST Levels of Care
Primary mental health care falls into Levels 1 to 4, with Level 5 being more appropriate for acute and specialist mental health services.
Level 1 (self-management) for people with relatively minor problems on the primary domains. Contraindications to Level 1 care include problems with engagement and severe problems in treatment/recovery history or very severe environmental stressors.
Level 2 (low intensity interventions) for people with mild problems in the primary domains, where these do not present in the context of significant problems on the contextual domains. Level 2 may also be suitable for people with moderate symptoms, but this is dependent on extent of presenting problems on other primary and contextual domains.
Level 3 (moderate intensity interventions) for people with mild to moderate symptoms/distress where these present in the context of significant problems on other domains. Level 3 is also proposed as suitable for management of severe symptoms where no significant problems are present on other primary domains.
Level 4 (high intensity interventions) for people with severe symptoms/distress, where these occur in the context of significant other problems (up to severe levels). Level 4 is not suitable for people with severe symptoms who present with very severe problems on either risk or functioning. Individuals referred with this array of presenting problems are suggested as best referred to Level 5 care.
Level 5 (for acute and specialist mental health services) for people who usually have significant symptoms (e.g. hallucinations, avoidant behaviour, paranoia, disordered thinking, delusions) and problems in functioning independently across multiple or most everyday roles (work, education, parenting, volunteering) and/or is experiencing:
- Significant risk of suicide; self-harm, self-neglect or vulnerability.
- Significant risk of harm to others.
- A high level of distress with potential for debilitating consequence.
Medicare Mental Health Hubs/Pop-ups/Centres
Consumers are eligible for services through the Medicare Mental Health-funded Centres (Hubs in Victoria and Pop-ups in NSW) for IAR-DST rated Level 3 and 4, and the consumer cannot afford or otherwise access similar services.
This could be based on one or more factors:
- Inability to afford a similar service such as Better Access
- Complexity of need and requiring a multidisciplinary team approach
- Location with respect to service availability
- Would not be better suited to a specialised service in their area of need i.e.: Victims of Crime Counselling and Assistance Program, Work Cover, TAC, Child First, Directline, Family Violence Services, Homelessness Services etc.
Where an IAR is completed with a consumer, and their needs are best met by a service other than the Mental Health Hubs, it is the role of the intake worker to support them to navigate to the most appropriate service for them.
IAR-DST Level 5 referrals
On completion of the IAR, where the person has been rated as a level 5, and/or:
A. If risk of harm is assessed as imminent;
- Wherever possible discuss your need to arrange an urgent/crisis referral with the consumer
- Obtain consumer’s first and last name, phone number and current location
- Refer consumer to 000 as appropriate and provide handover of pertinent information
- Inform supervisor / manager as soon as possible on the day of the contact.
B. If risk of harm is not assessed as imminent, the intake worker must;
- Discuss consumer’s support needs and risk level with worker’s supervisor / manager (see local guidelines/ practice guidelines).
- It may be appropriate to seek collateral information from providers currently involved in the consumer’s care to determine history of risk, and their assessment of the presenting needs for the consumer. The intake worker would need to consider the consumers presenting risk, and whether the consumers consent would need to be gained to engage with the wider care team. This consent will also need to be documented.
- Consider appropriate referral pathways
- Refer to local area mental health services as appropriate
There may be circumstances where a practitioner may assess that a Level 5 where an Area Mental Health Service intervention may not be appropriate.
Examples:
- Consumer is already well engaged with existing mental health support services i.e: psychiatrist or psychologist.
- Consumer is booked in to access these professionals within the next 48 hours or these professionals can provide support over the phone in the interim.
- Consumer has agreed to a safety plan and is agreeable to accessing these supports in the next 48 hours.
Clinical decision override
- Intake/Hub worker may choose to make clinical override judgment to step down from Level 5. The decision to over-ride a level 5 decision, must be discussed with a senior, the reasoning must be clearly documented why alternative practitioner rating was agreed upon and clearly annotate support and safety plan.
- Where possible, the original intake worker who took the call with the consumer is to call the consumer back to agree on support plan and support them to develop a safety plan for the next 24-48 hours (reference local safety planning processes). Schedule text message to be sent no later than 7 days later to check in on consumer’s progress. Clinician may assess that an earlier text message or a call may be more appropriate dependent on support plan in place.
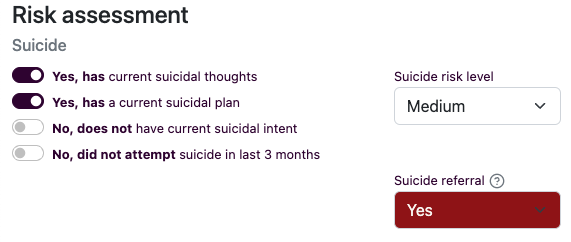
Suicide Referral
The Risk Assessment section includes a ‘Suicide referral’ flag. This flag automatically switches to Yes when the risk of suicide is assessed as medium or high, and/or the consumer has a suicide plan and/ or intent.
A referral with a suicide flag requires appropriate supports are put in place to help manage that risk and start a time check point for consumer follow up. That support will be dependent on the needs, and the circumstances for the consumer. It may be a referral to a tertiary health service, a referral to a rapid response service, or the increased support from currently engaged supports/ services.
Discuss referrals with a suicide flag with your supervisor to ensure appropriate care planning and engagement.
Where the referral is allocated to a Hub/Centre for their ongoing care, consumers must be contacted within 24 hours, to further assess risk, and engage them in care.